The industry leading software solution that enables cancer centers to provide coordinated navigation, distress management, and survivorship care planning
Equicare Health, Inc. Announces the Appointment of New Board Member
{Equicare names industry leading expert to help further advance the Equicare portfolio.}
Vancouver, BC Canada – October 28,2020. Equicare Health, Inc. announces the appointment of Christopher Hanna, Ph.D. to the Board of Directors. He re-joins long time colleagues, Greg Peet and Len Grenier, as the fifth member of the Equicare Board.
There is no denying cancer screening transformed cancer care, as it aims to detect cancer before the appearance of symptoms. Timely screening has proven to be an effective tool in early diagnosis and decreasing cancer mortality rates. With early screening and engagement, health professionals are able to connect with patients sooner and tailor treatment plans to individual screening results and tumor characteristics, ultimately enhancing patient outcomes.
This initial step in cancer care has been dramatically altered due to the global pandemic. The Centers for Medicare & Medicaid Services in the United States have classified screening as a low-priority service and suggest healthcare organizations to consider postponing screenings. Many patients are also fearful of exposure to the COVID-19 virus or of overburdening healthcare services and thus have been less likely to present to healthcare services for cancer screening and diagnosis. As a result, the number of tests to screen for cervical, breast and colon cancer fell by 85% or more after the first COVID-19 cases was diagnosed in the U.S..
The coronavirus disease (COVID-19) continues to spread globally at an alarming rate, influencing all sectors of our society. The burden of COVID-19 on health systems has important implications for cancer prevention and treatment, including:
DOI:https://doi.org/10.1016/ j.trecan.2020.04.005
an increased risk of infection for cancer patients,
the suspension of screening, and
the de-prioritization of other cancer care services, including diagnosis and treatment.
These changes have had and will continue to have a profound impact on the lives of cancer patients and their families, as well as care providers. Patients with cancer are known to be at increased risk for community acquired respiratory viruses due to their immunocompromised state, and are vulnerable to worse outcomes from the infection. They might be more likely to get infections because of the cancer itself, certain cancer treatment modalities, poor nutrition, and other co-morbidities. Patients are also worried about potential exposure to this infectious disease, and have been reluctant to seek health services out of fear that they will be exposed to the virus.
Vancouver, CANADA – April -, 2020. Equicare Health Inc., the leading provider in oncology care coordination and patient navigation solutions, introduces EQUICARE CONNECT, a secure, cloud-based video conferencing platform that allows clinicians and support staff to communicate with healthcare providers, patients and their families.
EMR’s: So Many, So Expensive, and So VERY Confusing
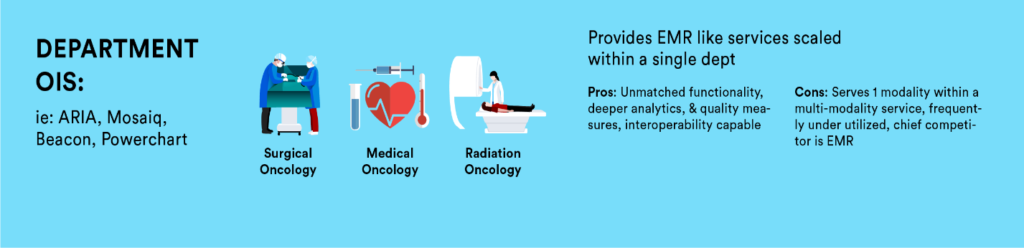
During our own professional careers, we have observed the rapid development of Electronic Medical Records (EMR) at various levels; from the wide enterprise level EMRs (Epic/Cerner/Athena/Meditech) that reach across hospitals and health systems to more specialized software that resides at a department level (ARIA/MOSAIQ/Beacon) and those even more granular at a functional level (Equicare/PACs/PowerPath) that provides specialized functionality not provided in other levels. Selecting a software involves a large range of influencers: CEO/CFO/CIO/Service Line Administrators, Department Director, clinical staff, physicians, nurses, and other ancillary staff with each having their own requirements influencing their choice. This complexity contributes to a somewhat less than ideal EMR infrastructure.
What does each individual care about? For a CFO, the cost savings associated with consolidation to a single enterprise level EMR is clear. For a CIO, an enterprise level EMR means fewer applications to manage, fewer resources to support, while also decreasing the risk for cyber vulnerability and record loss. Clinicians value the specificity to software while also the availability of information with fewer applications. Administration values reliability, availability of analytics/data, user satisfaction, costs, and other factors. In the end, no single person fully owns the outcome as there are numerous influencers and decision makers that weigh in with various and even competing expectations.
Enterprise level EMRs offer an opportunity to consolidate patient-related information into one centralized database. This alone is highly attractive as it provides a single source, high-level view of patient, clinical and financial information. Department-specific software provides functionality that enterprise level EMRs are simply incapable of, e.g. ARIA and Mosaiq. Both evolved from FDA approved Record and Verify systems that drove linear accelerators to become full departmental level information systems incorporating all treatment related activities that take place for a patient, such as: treatment schedules, simulation workup, treatment plan, billing, and consult/nurse documentation. As clinical care has become increasingly subspecialized, so have the tools to effectively manage. Functional level software is designed specifically to meet this increasingly complex demand that department and enterprise level are unable. For examples, a PowerPath software is necessary for tissue analysis while Equicare delivers end-to-end cancer care coordination including: interactive patient communication, screening, education, treatment summaries, and a comprehensive follow up plans. All of which are necessary when managing a chronic disease like cancer with efficiency and specificity. The value increases as we move away from a fee-for- service model and become more value based. This leaves us as oncology leaders to ask… what software do I really need to meet our goal of coordinating care for our patients and providing value-based care to our patients?
Rather than developing a comprehensive software plan that achieves our goals across departments, service lines, and even hospital networks, we often tackle software in silos not realizing the possibilities. Correcting this involves weighing the ambitions and vision of the organization with the financial expense, sensitivity to cyber security, and accepting the pain of implementing a software application plan.
The argument to consolidate and migrate all information to one enterprise level EMR offers great value on the surface. The issue with this, however, is that the scope of an enterprise level EMR is rather limited as no single EMR provides enough specificity to support and manage a complex service like oncology. The number of ongoing regulation and accreditation changes alone which must be kept current often creates a choice in labor intensive/inaccurate data or automated/accuracy. Our software tools provide the infrastructure we use to deliver care to our patients, yet we spend little time designing our platform. Most software applications do a good job within their scope and level; however, issues often arise when software is procured to do more than it is capable. Within our oncology space, this is a common occurrence. We should accept that this is less a fault of the software and more a fault of the organization implementing the software, as we are often asked and/or we attempt to utilize the wrong tool.
Here is an important factor to consider: once you have your software in place as designed, you are not done. You have consolidated in some areas and may add in others, need to address cyber threats, improved work flows, upgraded as entitled in service agreements, but still you have silo’d services. Everything we do in healthcare involves collaborating across services (adjuvant therapy). As our patients travel through the organization, our software should provide the infrastructure for their specific information to travel with them by being easily accessible to other care providers. This is only achieved via interoperability or establishing interfaces. When weighing software, value those that offer information exchanges with each other. Enterprise level EMR’s can offer bi-directional information exchanges with department level as well as specialized functional software. Not all information needs to convey, only what makes sense for patients, supportive services, providers and their referring network. Many software providers already have experience in identifying what data information is in demand, which is why they likely offer standard interface packages. Note, this serves as a starting point as each facility needs to identify what data they want to travel vertically and if up, down, or bi-directional. Additionally, you may need to specifically ask for the interoperability as the software provider likely prefers a consolidation to their own product or is not vested in an integrated solution ultimately serving our patients and network of providers.
Professional Opportunity
Within your organization, consider leading an initiative to organize your software so that it is aligned to the goals of your organization vertically. Ensuring it delivers horizontally within oncology on meeting security standards, reduces data-entry error/duplication, improved work flows for clinicians, access to data for analysis, accurate billing, timely scheduling, provides quality care coordination, patient education, data for accreditations, Patient Reported Outcomes (PROs), screening and long term Follow up plans. With senior leadership support, establish a small committee comprised of a representative from IT&S, clinical support, administration, fiscal/billing, quality, and risk management to drive the project. Below is a short list of suggested steps to begin with:
Set a comprehensive goal for delivering end-to-end cancer services:
Security (meets recognized standards)
Functionality (comprehensive care coordination from screening through survivorship)
Interoperability (create connectivity between functional, department specific, ancillary and enterprise wide EMR’s)
How many software applications do you operate within your service line?
List them and the functions you utilize as well as functionality not utilized
Are your current applications HL7 compliant?
Identify duplication
Are you due for upgrades per a service agreement that would enable additional functionality?
Identify redundancy where either toggling between or re-entering data
Review contract terms to determine if owed upgrades, training, and out clause.
Determine if you can consolidate?
What do you utilize one for that another can do, maybe not do as well, but meets a standard? Consider the cost of errors if you plan to expose yourself to a manual process over an automated one, as well as the staffing resources for duplicate entry.
Are you remaining current with your upgrades and would newest versions provide additional functionality?
Is there a gap in what you have that cannot be made with existing software?
Do you have IT&S staff who understand the products and have relationship with the vendors?
Consider the safety implications of a patient presenting at an ER if the upstream EMR cannot adequately display what the patient’s previous treatment regimen has been.
Is your IT&S staff capable of testing and implementing the required interfaces.
What opportunities are there for bi-directional information exchanges through a set of standard interfaces?
Can cost be bundled into purchase agreements?
Can cost be amortized?
Is it a capital or operational expense?
When you have selected the software design that supports your goals, work towards them understanding it will take time while remembering the value of integrated software applications. Existing contracts do not limit our ability, only the timeline and you may find you are owed upgrades and training. Do not simply purchase the cheapest software or the “best” software; rather, take time to identify what software is best for your organization given the level where it will reside with others along the vertical environment.
Summary
When a cancer program offers true care coordination across the service line, a byproduct is reduction in duplication, data-entry errors, missed billing, less toggling, better engagement between physicians-patients-departments, less volume leakage, more efficient passage through services, reduced cyber threats, increased staff capacity, adherence to Evidenced Based Guidelines (EBG), Patient Reported Outcomes (PRO), and a more streamlined patient centric approach. Regardless of what level the software resides at, the selection should not be a decision made in a vacuum. Rather, a multi-year strategic plan that leads to an agreed upon goal while understanding the value of leveraging your software together through information exchanges and interfaces.
In the end, providing comprehensive end to end cancer services that integrate with all EMR levels to deliver evidenced based guidelines, gain efficiency through automation and increases synergy between service lines, should be our goal. This means your functional software solution should coordinate patient care beginning with screening, managing the workup phase, seamlessly connect to multi-modality treatment care, inpatient/outpatient care, registration(s), billing, portal, and smoothly transitioning a patient through survivorship. Ideally, care coordination software will do all this and exchange the meaningful information with horizontal enterprise level EMR’s, ancillary support tools, i.e. pathology, radiology, etc… as well as department specific support tools, i.e. radiation, medical and surgical oncology information systems. Remember the winner is not the software that does it best, the winner is the patient with a SW that does interoperability both vertically and horizontally the best.
Cancer is not just one disease, it encompasses many variations of disease. The term cancer is commonly used for diseases where abnormal cells divide in an uncontrolled manner and may invade other tissues and parts of the body through the blood and lymph system. Cancer can take years, or sometimes decades to develop.
In the United States, one in four people develops cancer at some point in their lives. A cancer diagnosis can have devastating effects on the patient, their families, and the greater community. With the rates of cancer expected to increase, its burden on society, in terms of lost productivity, and costs of treatment and care, will exacerbate.
Extensive research has shown that the risk of cancer depends on a combination of multiple factors: behavioral, genetic and environmental. Anything that increases the chance of developing cancer is called a cancer risk factor. There are also some factors that play a protective role in cancer development. Some of these factors are modifiable or controllable, while others are not. For instance, smoking cigarettes is a modifiable risk factor as a person can control their exposure.
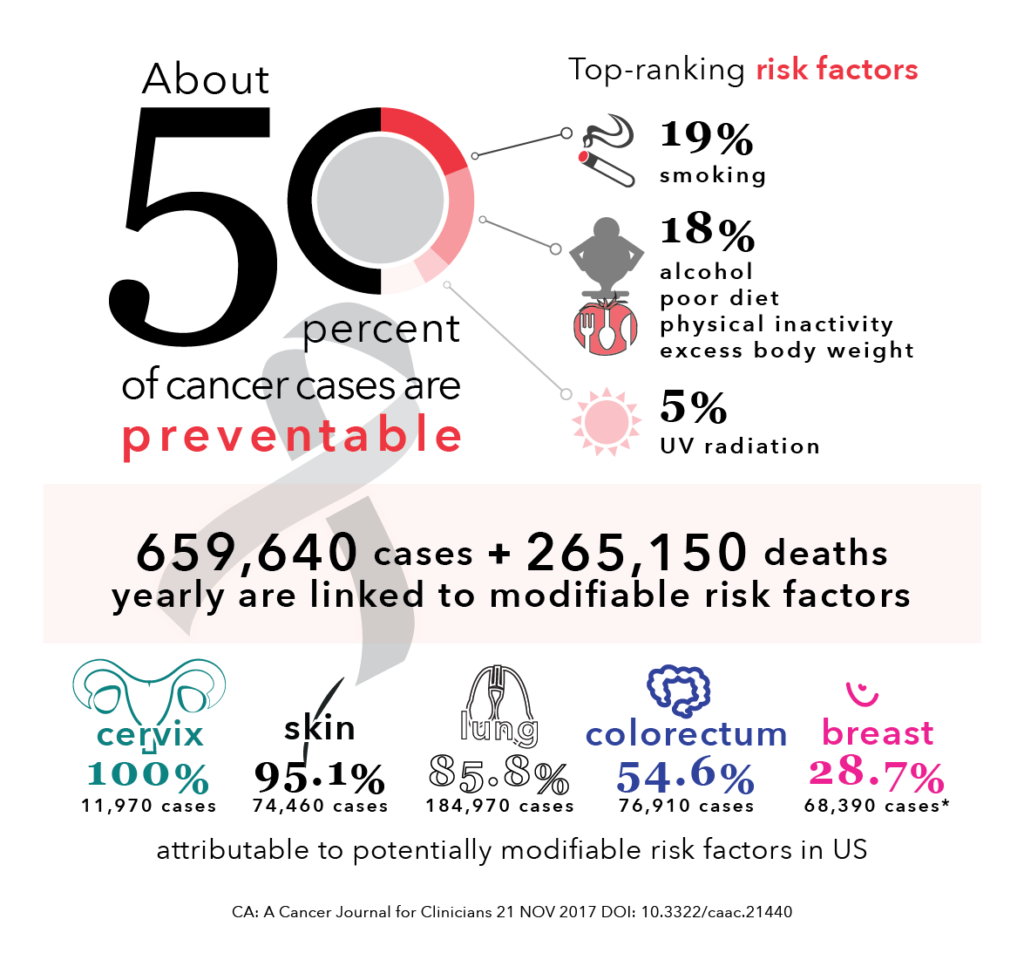
The American Institute for Cancer Research has reported that nearly 50% of common cancer cases are preventable [1]. Cancer prevention is any action taken to lower the chance of getting cancer. With the rates of cancer increasing, prevention is more important than ever to curtail cancer incidence. Primary prevention through behavioural interventions – commonly referred to as ‘lifestyle’ interventions – are the most cost-effective long-term strategy to reduce the burden of cancer and lower the number of deaths caused by cancer [2].
Here, we will review some major modifiable lifestyle factors that influence cancer risk. There are a set of factors that are known to increase the risk of cancer, such as:
1. Cigarette smoking and tobacco use
Tobacco is the single greatest controllable risk factor for cancer mortality, causing about 30% of all cancer deaths in the United States [3]. Tobacco use is associated with an increased risk of many different kinds of cancers, from bladder and cervical to esophageal and lung. A smoker’s risk of cancer, depending on how long a person has smoked, can be two to ten times higher than a non-smoker’s risk [4].
Exposure to second-hand smoke, also known as environmental tobacco smoke, also increases the risk of cancer and other diseases. The smoke that is exhaled by smokers or created through the burning of tobacco products contains the same cancer-causing chemicals as those inhaled by smokers. Recent evidence has also shown that residual nicotine and other chemicals left on indoor surfaces by tobacco smoke, known as thirdhand smoke, is hazardous and contains cancer causing compounds.
Not smoking or quitting smoking dramatically lowers the risk of cancer diagnosis and death. People of all ages can improve their health by quitting smoking. People who quit smoking decrease their risk of lung cancer by over 30% after 10 years, compared to smokers. The risk of mouth or esophagus cancer is cut in half within 5 years after quitting [5].
For cancer survivors, the effects of smoking are even worse: there is an increased risk of cancer recurrence and negative long-term side effects from cancer treatment. Electronic software tools, such as EQUICARE CS™ (ECS), can facilitate this process by providing lung cancer screening forms and guidance to smoking cessation aids.
2. Radiation
There are two main types of radiation that are associated with an increased risk of cancer: ultraviolet (UV) and ionizing radiation.Ultraviolet (UV) radiation from sunlight is the main cause of nonmelanoma skin cancers. UV-emitting tanning beds have also been classified as carcinogenic. Sunscreen and protective clothing are effective preventive measures.
Ionizing radiation is released from medical radiation tests (e.g., x-rays and CT scan) and radon gas present in homes . Radiation used in medicine can be impactful in helping save lives as well as preventing the need for more invasive procedures. However, inappropriate or excessive use may cause harm to patients. Residential exposure arises from radon, a naturally radioactive gas sometimes present in soil, and can increase risk of lung cancers.
3. Infections
There are certain infectious agents (viruses and bacteria) that are cancer-causing. In2012, approximately 15% of all cancers were attributable to infectious agents [6]. These viruses and bacteria include:
Human papillomavirus (HPV) that
increases the risk for cancers of the cervix, penis, vagina, anus, and
oropharynx
Hepatitis B and hepatitis C viruses that increase the risk for liver cancer
Helicobacter pylori that increases the
risk of gastric cancer
Vaccines have been developed, and approved by the Food and Drug Administration, for the prevention of two of these cancer-causing agents: hepatitis B virus and human papillomavirus (HPV). These two vaccines can reduces the risk of liver and cervical cancers, respectively.
Conversely, there are factors that may affect the risk of cancer. Nearly all of the evidence linking these factors to cancer risk come from observational studies. Data from observational studies is powerful as it gives researchers insight about relationships between potential factors and cancer risk. However, such studies cannot definitely establish a cause-and-effect relationship as their influence is complex and multifaceted. These modifiable factors include:
1.Alcohol
The harmful use of alcohol is a serious health burden, and affects all individuals globally. Risky alcohol intake kills 3 million people every year [7]. Alcohol intake is a risk factor for many cancer types: oral cavity, pharynx, larynx, liver, colorectal, and breast. There is a dose-response relationship between the risk of cancer and alcohol consumption: risk of cancer increases with the amount of alcohol consumed.
2. Physical activity Physical activity includes any action that requires more energy than resting – working, exercising, and leisure activities. It is essential to maintain a balance between the calories consumed and used. There is substantial evidence that physical inactivity is linked to higher risks of several cancers [8].
The association between colon cancer and physical activity has been extensively studied. It has been found that most physically active individuals have a 24% lower risk of colon cancer, compared to those who were the least physically active [9]. With regards to breast cancer, many studies show that physically active women have a lower risk of breast cancer than inactive women. A meta-analysis has shown that the average breast cancer risk reduction associated with physical activity was 12%.
Physical activity has a number of biological effects on the body that help to explain associations with specific cancers. For instance, exercise can lower hormone levels and certain growth facts that are associated with cancer development and progression. Exercise can lower the risk of 13 specific types of cancer. There are also beneficial effects for several aspects of cancer survivorship [10], such as weight gain, quality of life, cancer recurrence or progression, and prognosis. [MD16] The American Cancer Society recommends that adults get at least 150 minutes of moderate intensity or 75 minutes of vigorous activity each week. [11]
3. Diet
The link between diet and cancer is as cryptic as the disease itself. For years, research has pinpointed certain foods and nutrients that tend contribute or help prevent certain types of cancers. There are four subgroups that standout:
Processed meat is any meat that has been smoked or fermented or includes added salts and nitrites – associated with an increased risk of cancer.
Glycemic index (GI), a measure of how fast carbohydrates turn into sugar in the blood, can help identify the whether certain carbohydrates are protective or detrimental for health. Consuming foods with a high GI (sugary drinks and processed foods) is associated with an increased risk of prostate cancer [12]. Conversely, eating lower-GI foods, such as legumes, with associated with a 30% lower risk of both prostate and colorectal cancers.
Antioxidants play an important role for cancer prevention since assist in neutralizing free radicals that can damage cells.
Calcium may be a protective or a risk factor for certain cancers.
Some of these strategies mentioned are an effective alternative for preventing a larger burden of chronic disease worldwide, including cancer. Exposure to these factors is preventable. Through reducing exposure to these modifiable risk factors, 694,000 cases of cancer could be prevented in the United States every year [13]. It is important to note that there are things that can be done today to help prevent, delay, or even stop the cancer process.
Written by Dorri Mahdaviani , who holds a Masters of Public Health (MPH) from the University of British Columbia (UBC). Her academic and professional interests include the areas of chronic illnesses, health care systems and childhood health and development.
Infographics and Design by Ann Wong, who holds a PhD in Biochemistry and Molecular Biology from the Faculty of Medicine at the University of British Columbia (UBC), Canada. She is an author of over 10 SCI publications, having taught at UBC and the Peking University Health Science Center (PUHSC) in Beijing
Vancouver, CANADA – April 9, 2019 – Equicare Health, the leading provider of oncology care coordination and patient navigation solutions, officially released the latest version of their product, Equicare CS (ECS) 4.10.
“ECS 4.10 adds a number of new
features that make it easier to collect and monitor Patient Reported Outcomes
as part of standard clinical practice. The release also includes patient
navigation workflow improvements, and GDPR support for our customers in the
European Union,” says Malcolm Wright, VP of Product Management at Equicare
Health.
Consumerism is one of the greatest driving forces behind innovation. We live in a world where markets focus on the needs and wants of consumers, and the health system does not deviate from this trend. To meet the demands of rising health-related costs and complexity, for patients and health administrations, operational changes have started taking place.
Technological advances are the key to instigating operational shifts in the healthcare marketplace. In this piece, we will explore a few overarching barriers within healthcare, and how emerging innovations aim to circumvent barriers for individual patients and the entire health system.
1. Building engaging relationships
Relationships are an integral part of the health system. While the doctor-patient relationship is very important and key to effective health care, it is not the only relationship that matters. There are many points of contact in the health system where communication falls short due to ineffective engagement. Points of contact in healthcare are normally between:
Physician and Patient
Administrative staff and Patient
Physicians
Physician and Caregivers/family
Physician and Allied health professionals
Digital health tools can be used to facilitate communication,enhance engagement and bolster relationships. They are about reinforcing and improving the relationship within healthcare, particularly between patient and healthcare providers. Three-quarters of physicians have linked improved patient engagement with digital patient engagement tools, and the majority of physicians had a form of digital education tool in their clinics [1].
Engagement cannot be measured by the initial interaction to a digital tool. If engagement is to be effective, it has to be sustainable. To ensure sustainability, digital tools aim to also impact methods that are of concern for the health system: automation, workflow integration, and provision of actionable data. In essence, consumers, both patients and health administrators, value experience, and have come to expect personalized, targeted approaches to address problems.
2. Data management
Patients have been and continue to receive care across multiple health sectors, from primary to acute care. Electronic health records (EHR) tools have been put in place to facilitate the collection of data in healthcare settings. Unfortunately, healthcare providers and organizations continue to utilize fragmented technologies, creating barriers towards collaboration and data sharing opportunities. These barriers are worsened if a patient utilizes both public and private healthcare resources. The information gathered at each interaction with the health system needs to be managed and stored in a manner that can be utilized in the future. To date, artificial intelligence (AI) and machine learning have made incredible impacts on the practice of digital healthcare. In 2019, further advances in the move toward seamless care are expected.
As more data feeds into health systems, further advances need to take place to ensure efficient care and the ability to implement solutions are achieved. Standardized software implemented in healthcare settings must provide the technological foundations for data sharing — extending the functionality of EHRs and other technologies that support connected care. Interoperability is a major component in digital health innovation: as health data is received from multiple sectors, secure data exchange becomes imperative in providing continuity of care. With interoperability, data can be aggregated across multiple providers and settings. Applications that target hospitals and medical clinics will include patient monitoring and transcribing notes for EHRs. Lastly, complete access to EHRs for patients and providers is an essential step in the push toward providing a holistic picture of a patient’s health profile to themselves and any care provider resulting in enabled targeted health outcome.
3. Meeting the demands of integrated care
Chronic diseases, like heart disease, cancer, stroke, or diabetes, are the leading cause of death and disability in America. 60% of Americans have at least one chronic disease, accounting to over 80% of hospital admissions [2]. These patients and their care need to be managed. Management of chronic illness is one of the key areas of growth in 2019, along with behavioral health and specialty medicine. These needs range from annual wellness exams to the opioid crisis, where healthcare providers are at the forefront to addressing these demands.
Platforms and applications that are interoperable with EHR systems will be especially valuable to providers across all health sectors, given the increase in insight and communication telehealth will provide about a specific patient. With limited resources in the health system, from financial constraints to continued demands of regulatory compliance and accreditation, enhanced clinical efficiency via digital health tools will make it easier for healthcare providers to provide care. Integration of such platforms provides physicians with the ability to monitor vital signs and assess reactions to treatments without being physically present while providing real-time diagnosis and intervention without time-consuming office visits.
Through the provision of clinical care at a distance, increasing accessibility and eliminating potential delays in care has and will give patients greater control, thus enhancing satisfaction and overall engagement.
Digital health now has successfully expanded to include support for a wide range of conditions across the spectrum of care, from behavioral health to cancer, heart conditions, and other complex care conditions. As health systems increase their focus on value-based care and population health, these tools will provide convenient and lower-cost opportunities to access care.
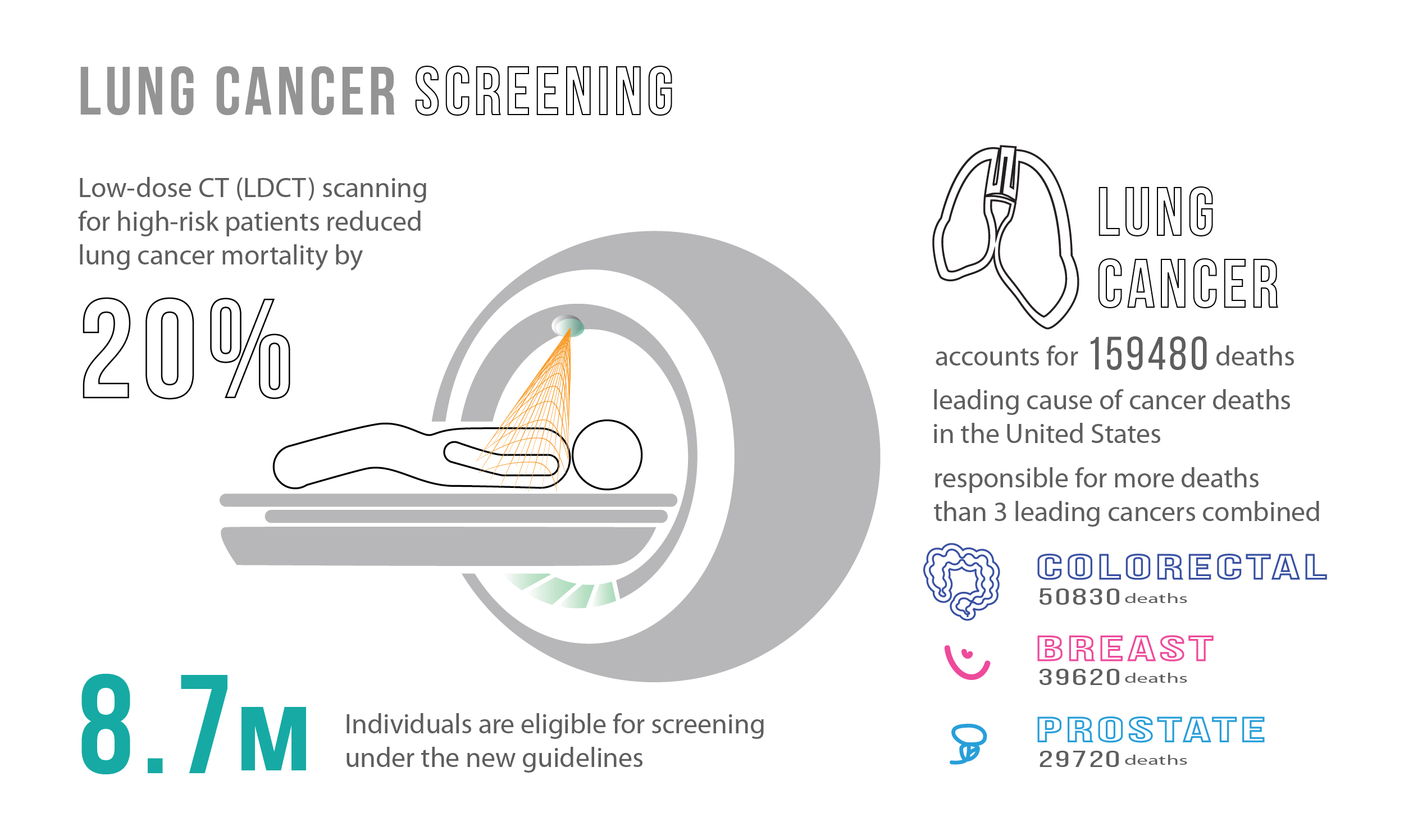
Lung cancer is the leading cause of preventable cancer deaths worldwide, with over 1.5 million deaths per year. It claims more lives each year than colon, prostate, ovarian, and breast cancers combined [1]. It is a complex disease and usually considered as a result of smoking effects and multiple genetic variations. To add to this, lung cancer has a poor prognosis, with no major improvements in the 5-year survival rate for the past 30 years [2].
In the United States alone, an average of 425 people die from lung cancer each day [3]. When looking at lung cancer statistics and distributions, monitoring and surveillance is recommended for women as development rates are disproportionate between men and women. Mortality rates are projected to increase significantly in the coming years. Women are one-and-a-half-times more likely than men to develop lung cancer, and those who have never smoked are more likely to develop lung cancer when compared to men who have never smoked [4]. Controlling for age, the global lung cancer mortality rate among women is estimated to increase by over 40% from 2015 to 2030 [5].
Having explored the current burden of disease, let us better understand risk factors and the complexity of lung cancer, along with promising interventions to aid and curtail this disease. There are a number of factors that may increase the chance of getting lung cancer, some are controlled and others are uncontrollable [6].
Controllable risk factors:
There is a dose-response relationship between the risk of lung cancer and smoking: the risk of lung cancer increases with the length of time and number of cigarettes smoked. Quitting, even after smoking many years, can significantly reduce the chances of developing lung cancer.
Second-hand smoke exposure. Smoking causes lung cancer by damaging the cells of the lung. When cigarette smoke is inhaled, whether it be first or second-hand, the lung tissue changes almost immediately. With each repeated exposure, the damage causes cells to behave abnormally, creating tumor cells.
Radon gas exposure. Radon is naturally occurring, and its radioactive gas is created from the decay of uranium in minerals present in rock, soil and water. Radon is the leading environmental cause of cancer, the leading cause of lung cancer in non-smokers and the second leading cause of lung cancer in smokers. The World Health Organization estimates around 14% of all lung cancer deaths globally are due to radon exposure. This represents 225,000 of the 1.5 million people that die annually from this disease [7].
Asbestos and carcinogens exposure. Asbestos and other carcinogens – such as arsenic, chromium and nickel – can increase the risk of developing lung cancer, particularly for smokers.
Uncontrollable risk factor:
Family history. Individuals with a parent, sibling or child with lung cancer have an increased risk of the disease.
Unfortunately, there is no guaranteed way to prevent lung cancer. Only risk factors can be controlled to mitigate their effects. Strategies to reduce risk include stopping smoking, avoiding second-hand smoke, testing living environments for radon, avoiding carcinogens, and living a healthy lifestyle.
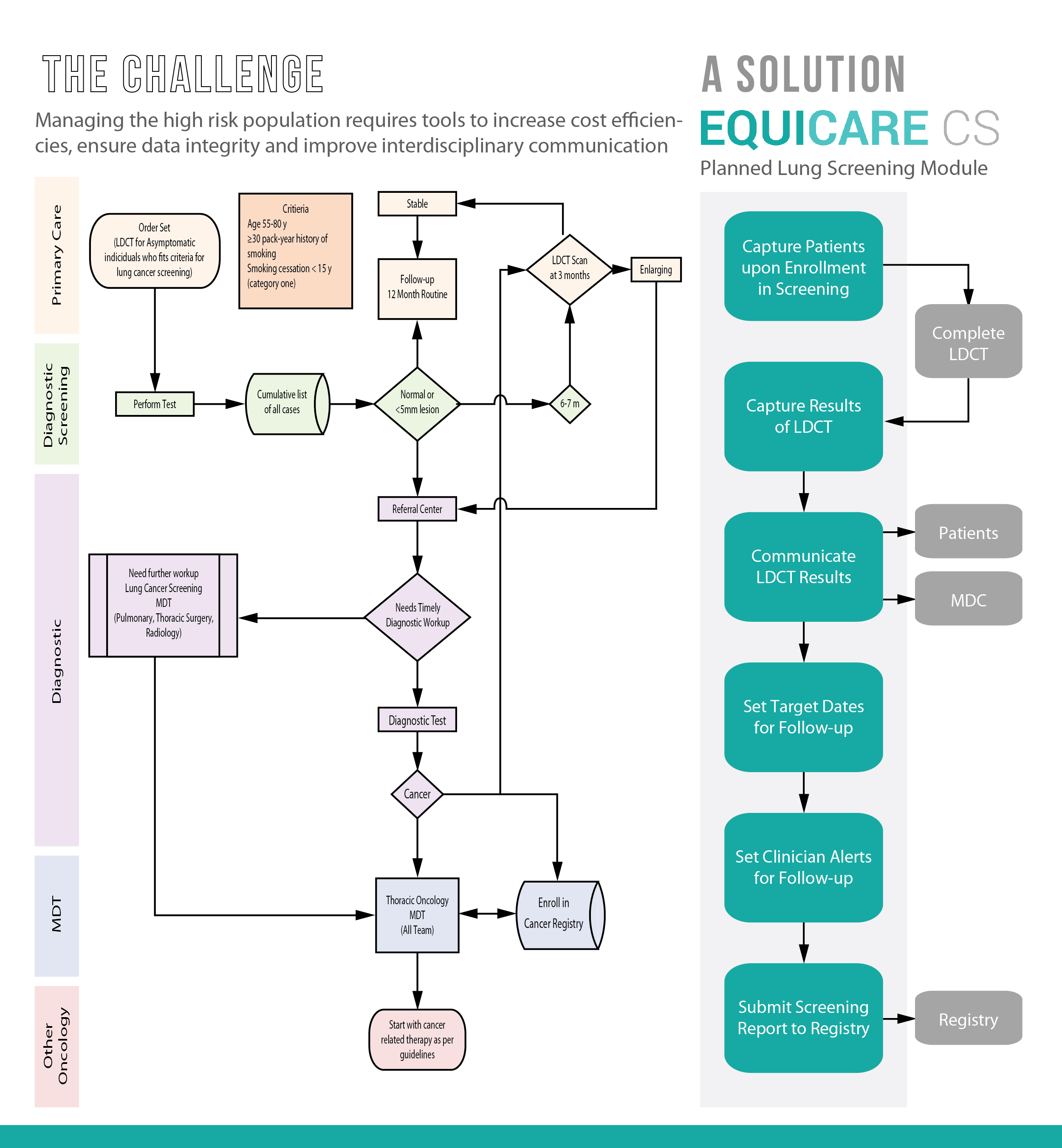
The complexity with lung cancer is that it typically does not cause signs and symptoms in its earliest stages. Individuals at risk of getting lung cancer should screen for the disease regularly. The US Preventive Services Task Force recommends annual screening for lung cancer in current and former smokers aged 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years [8]. Note that smoking is the number one risk factor, but it is not the only one. To reduce the burden of disease, a screening test must be able to detect lung cancer at an early stage to allow prognosis modifications, present a low percentage of false-positives, minimize adverse effects (i.e., cancer-induced radiation), and be cost-effective for the health system.
Currently, the most effective method to screen for lung cancer is through low-dose computed tomography (LDCT). LDCT is a unique CT scan technique that computerizes x-ray equipment to produce multiple, cross-sectional images or pictures of the lung. This screening tool has many benefits, including [9]:
reduced deaths from lung cancer by 20% for high-risk patients [11]
a lower radiation dose than standard chest CT scans
ability to locate smaller cancers compared to x-rays.
There is variability in cancer, and lung cancer is no exception. Lung cancer is typically divided into two major types based on the appearance of its cancer cells. Treatment decisions are then made by the healthcare team based on the type of cancer diagnosed. The two types of cancer include:
Small cell lung cancer (SCLC). This type is a less common type of lung cancer (about 10% – 15% of all lung cancers) [12] and occurs almost exclusively in heavy smokers. SCLC is a cancer without a specific treatment and often spreads early. Traditional treatment methods, such as chemotherapy, radiotherapy, and surgery allow about 6% of patients to survive five years post-diagnosis. Recently, researchers have gained insights into gene activity in human SCLC tumors [13]. This finding will allow for the development of personalized medicine approaches to target this form of lung cancer.
Non-small cell lung cancer. This type encompasses several lung cancer types that behave in a similar way, these include squamous cell carcinoma, adenocarcinoma, and large cell carcinoma.
Currently, the main modalities of lung cancer treatment include surgery, radiation, and chemotherapy. Similar to other cancers, early stage lung cancer is treated with surgery (e.g. video-assisted thoracoscopic surgery and robotic surgery), and more advanced cases are managed with chemotherapy and/or radiation therapy. Typically, a team of specialists from different fields work together to determine the most appropriate treatment options for the patient. The care team may include various types of oncologists, pathologists, nurses, pharmacists, and health administrators. Having a multidisciplinary team is especially beneficial when it comes to coordinating complex treatment protocols involving multiple therapies.
There is continuing efforts to improve the survival of patients with lung cancer, focusing on achieving an earlier diagnosis along with developing new targeted or personalized therapies for this disease. The International Association for the Study of Lung cancer has recently highlighted the importance of immunotherapy, a form of personalized medicine and an encouraging treatment method to fight against lung cancer. Lung cancer patients who respond poorly to standard chemotherapy now have more options: most recently two immunotherapy drugs were approved by the U.S. FDA for lung cancer therapy. Even though the survival rate for many lung cancer types still remains low, new targeted therapies and immunotherapies have the ability to change these statistics and are providing new hope.
Written by Dorri Mahdaviani , who holds a Masters of Public Health (MPH) from the University of British Columbia (UBC). Her academic and professional interests include the areas of chronic illnesses, health care systems and childhood health and development.
Infographics and Design by Ann Wong, who holds a PhD in Biochemistry and Molecular Biology from the Faculty of Medicine at the University of British Columbia (UBC), Canada. She is an author of over 10 SCI publications, having taught at UBC and the Peking University Health Science Center (PUHSC) in Beijing
Vancouver, CANADA – Nov 1, 2018 – Equicare Health, the leading provider of oncology care coordination and patient navigation solutions, is pleased to announce that it has been recognized as the 59th fastest growing company on the list of the Top 100 Fastest Growing Companies by Business in Vancouver (BIV) for British Columbia.
“We would like to thank Business in Vancouver for this award for a fourth year. This recognition is a constant encouragement for our team at Equicare who continues to innovate and find new solutions in delivering cutting-edge solutions in oncology care coordination,” says Len Grenier, CEO at Equicare Health.
Equicare Health was previously recognized in the 2013, 2015 and 2017 BIV Top 100 list.
About Equicare Health Equicare Health is the industry’s leading provider of comprehensive care coordination solutions. Equicare’s flagship solution EQUICARE CS™ (ECS) is a Multi-facility web-based software tool that facilitates patient engagement including patient-reported outcomes, patient navigation, survivorship care and a number of other clinical tools, i.e. MDT, Clinical trials, a suite of educational material, etc.. In additional to the clinical toolset, Equicare also offers an administrative suite of worklists and reports for managing adherence to accreditation standards including Meaningful Use, Commission on Cancer (CoC), NAPBC, QOPI, OCM, etc… ECS enables cancer centers to influence clinical outcomes for patients, optimize revenue streams, and increase operational efficiency. www.equicarehealth.com